|
There are many instances where riders seem to be unaware that their horse is lame as they ride or compete. Lameness is sometimes subtle and can be hard to identify as it may be a few missteps in the corner or during a transition or just that it ‘feels off’ to a rider who knows their horse well. Perhaps the horse’s back feels tight, the trot diagonals don’t feel even, or there is a reluctance to turn in either direction.
While lameness in horses cannot be prevented, it can be minimised when we understand the factors involved in its development. Horse owners should educate themselves in the most common lameness conditions that affect their horse’s breed, type, conformation, and discipline.
Learn about the relationship between conformation and lameness and work with your farrier to match conformation to use, hoof care and shoeing.
The ability of riders and trainers to recognise and acknowledge gait abnormalities in horses appears to be limited, commented The Centre for Equine Studies at Britain’s Animal Health Trust, citing several studies in a 2017 review.
Dr Jennifer Stewart addresses the subject of lameness.
Lameness can be a sign of pain, mechanical restrictions or neuromuscular disease. Defined simply as ‘…an abnormal stance or gait caused by either a structural or a functional disorder of the locomotor system….’, it can be hard to identify, detect and diagnose.
The most common problem in horses, lameness can be caused by nutrition imbalances, trauma, congenital or acquired disorders, infection, metabolic disorders, or nerve, cancer and circulatory system disease. Mechanical restrictions include upward fixation of the patella (inability to flex the affected limb), scar tissue in muscle (fibrotic myopathies) and restrictions caused by annular ligaments, adhesions and fibrosis (scar tissue). Only when an accurate diagnosis is made can the best treatments be chosen.
Factors that increase the risk of lameness in your horse include physical immaturity; developmental orthopaedic disease (e.g. OCD and limb deformities); poor conformation; improper hoof balance or shoeing; failure to adequately condition performance competition horses; repetitive stresses on bones, tendons, ligaments, and joints in performance horses; hard, slippery, or rocky work or paddock surfaces and extremely athletic activities. Inciting factors include trauma, fatigue resulting in incoordination of muscles, inflammation, infection, and failure to recognise early disease before it creates significant pain.
Just because there are no obvious signs of lameness doesn’t mean it does not exist - it can be very subtle.
When lameness does occur, you should contact your veterinarian promptly as this early examination can save you time, money and frustration by diagnosing and treating the problem immediately, possibly preventing further damage. The goal of early examinations is to keep small problems from becoming big ones. Pain is the most common cause of lameness in all horses.
Pain-related lameness can be weight bearing or non-weight bearing (swinging leg or ‘3-legged lame’) – and sometimes both are present.
We can all identify lameness when a horse is obviously limping - the head nod associated with forelimb lameness and the sacral rise, also called a pelvic rise or hip hike, associated with hindlimb lameness. But lameness may cause only a subtle change in gait, behaviour problems or a decreased ability or willingness to perform. Other times, it may only result in sweating or an increased heart rate at rest and during recovery.
The compensatory ways in which horses adapt to pain-causing lameness are complex and incompletely understood. This is especially so when there is more than one lame limb. Complicating the picture is that lameness in one part of a limb often results in secondary soreness in another part of the same limb, or in lameness of the opposite side (contralateral) or same side (ipsilateral) limb due to the horse compensating for the initial soreness by over-loading other areas.
A front leg lameness can decrease push-off and increase the pelvic movement asymmetry associated with the opposite side hindlimb. This compensatory load redistribution can be perceived as lameness. What this means is that even if the primary cause or source of lameness is obvious, your veterinarian may examine the whole horse.
Pain in any muscle, ligament, tendon or bone can cause lameness.
Because treatment varies greatly depending on the cause, it is critical to correctly determine the reason for the lameness. Unfortunately, many causes of lameness do not produce a characteristic gait abnormality, making diagnosis a challenge and frequently requiring a complete veterinary lameness examination. It’s important to call your vet when the horse is showing signs of lameness – if it’s been rested or spelling for a period of time it makes it difficult to evaluate your horse for lameness if it’s not lame anymore. Early examination and diagnosis also helps prevent progress of a simple ailment to a serious veterinary condition (e.g. foot abcess becoming osteomyelitis).
A horse can become lame for a range of reasons involving almost any part of the musculoskeletal system. Some conditions are more easily diagnosed and treated than others, so for equine veterinarians, lameness diagnosis and treatment is both science and art.
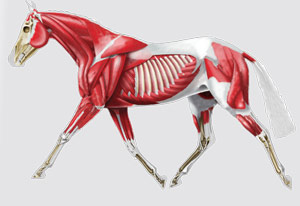
It requires a solid understanding of equine anatomy and physiology, conformation, biomechanics, pathology and medicine. Pain causing lameness can arise in any part the body that contains nerve endings.
Pain from skin wounds, connective tissue bruising, muscles, arthritis (joint inflammation), tendon sheath and bursal inflammation, tendon, ligament and bone injury can all result in lameness that cannot be differentiated by observing the horse’s gait.
CONFORMATION
Conformation correlates directly with the mechanical function of the limb and particular conformation characteristics can predispose a horse to particular lamenesses. Horses with poor conformation are more likely to experience problems with feet, joints, tendons and ligaments than are horses of ‘normal’ conformation.
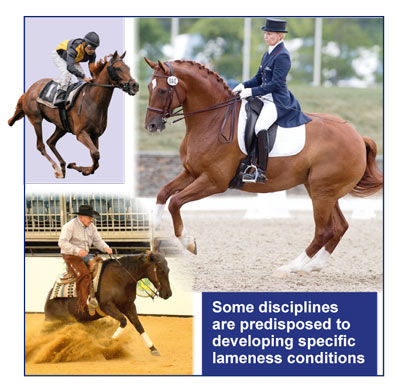
Certain breeds and disciplines are also predisposed to developing specific lameness conditions - knee arthritis in racehorses, hock arthritis in cutting horses, and hindlimb suspensory lameness in dressage horses.
The site and nature of the problem cannot be determined with certainty by the appearance of the lameness or the way the horse moves.
Front leg lameness (most of which arises in the foot in the adult horse and rarely in the upper leg) is easy for most people to recognise.
Hindleg lameness is more difficult - especially subtle upper hindlimb conditions. And, the huge muscle mass on the hindquarters makes it harder to see and feel deeper structures, and more difficult to image these structures using radiographs and ultrasound.
LAMENESS EVALUATION
Veterinarians are trained in the specific systems for performing examinations, which may include: medical, exercise and feeding history; visual of conformation, balance, weight-bearing and physical abnormalities; evidence of injury, stress or previous surgery to muscles, joints, bones and tendons; hands-on assessment for evidence of pain, heat, swelling anywhere; evaluation during walking and trotting in a straight line, on a hard surface, a circle, a round yard, lungeing and under saddle, and joint flexion tests. In some cases the speed and concussion of a faster pace (canter or gallop) is needed for the lameness to appear. Based on the history and physical examination, further diagnostics could be necessary.
The first step in a lameness evaluation is a thorough history. Often overlooked is the basic need to have a balanced calcium to phosphorus ratio. An imbalance leads to osteoporosis (commonly called ‘big-head), and the associated lameness is often shifting – i.e. it seems to move from one area to another – intermittent and difficult to diagnose.
Diet analyses have shown many horses on standard, typically normal feedstuffs and diets have an unbalanced ratio – especially if there is no lucerne in the diet. The most common cause, however, is grazing high oxalate grasses. Oxalates are chemicals more abundant in warm season grasses - such as buffel, setaria, green panic and kikuyu grass - that latch onto calcium making the calcium unavailable for the grazing animal to utilise.
The resulting osteoporosis, defined as a disease affecting horses, that may cause distortion of the bones of the head, and frequently lameness, can affect ligaments, tendons, joints and bones throughout the whole body and hence the presenting signs vary and are often misdiagnosed. Diet analysis is critical.
Because the best treatment depends on correct diagnosis, additional procedures are often necessary to isolate the specific location and cause of lameness. The veterinarian may recommend further tests, including diagnostic nerve or joint blocks, radiographs, nuclear scanning (scintigraphy), ultrasound, arthroscopy or examination of blood, synovial fluid and tissue samples.
Nerve and joint blocks are often our most important tools to identify the location of lameness. Working systematically, specific regions are anaesthetised, until the lameness disappears, enabling isolation of the area of pain, and helping determine whether the condition is treatable. Radiographs are useful in identifying damage or changes to bony tissues, however not all Xray changes are a cause for concern, and little information is gained on structures inside the joints such as tendons, ligaments or synovia (the membrane lining the joint), which are often the source of lameness.
Scintigraphy (nuclear scanning) involves injection of the horse with a radioisotope, which concentrates in sites of injury. The site can then be located with a gamma camera.
Thermography, MRI, CT scan and ultrasound provide information on blood flow, images of internal structures and their dimensions, and the presence of fluid, tears or other abnormalities can be identified.
Arthroscopy usually requires general anaesthesia and allows us to look into joints and tendon sheaths, and if necessary, surgery can be performed at the time. Blood, synovial (joint) fluid and tissue samples can be collected for laboratory examination and detection of abnormal cells, infection or inflammation.
There is endless lameness information on the internet, some of which is reliable and useful. But the first thing is to have a proper diagnosis, which only a trained and experienced veterinarian can provide. All of the above steps, when performed properly and assembled and interpreted correctly, help to provide an accurate diagnosis and form the basis for a treatment program.
The definition of lameness is simple enough! But sometimes it is too simplistic because whether or not lameness is readily apparent, the quality of equine performance can be influenced by pain. There are some horses in which pain-related abnormalities of gait are only observed as a compromise in quality of movement, which may be most obvious in canter. Recognition of low-grade lameness or multi-limb lameness is not always simple: if more than one leg is involved, the horse may just perform less well than previously; if nerve blocks remove one source of pain, obvious lameness may appear in another limb. Recent techniques using inertial sensor-based systems, global-positioning systems, motion-capture, force plates and movement analysis are advancing our ability to identify and localise subtle gait changes.
SADDLE FIT AND LAMENESS
‘Bridle lameness’ is linked to asymmetric rein contact, an imbalance between the rider’s hand and leg, or insufficient ‘straightness’ training. There is a similar relationship between the horse’s legs, the rider, the saddle and the back (also called thoracolumbosacral function). Lameness, thoracolumbosacral pain and reduced range of motion often coexist. Saddle-fit for both horse and rider is crucial for optimal thoracolumbar health and function. Saddle slip is usually blamed on saddle fit, crooked riders or horse shape, but persistent slip of the saddle to one side is most often caused by a back leg lameness. Shoeing also affects equine locomotion - especially in hindlimbs. The importance of an experienced farrier cannot be over-stated.
Sub-clinical laminitis – where the lameness is not severe enough to present as a definite or readily observed symptom - is a relatively common syndrome.
Sub-clinical in that, although detectable on xray, there are no clinical signs and no hoof-tester response. However, when travelling at speed the load through the front hooves and pedal (coffin) bone is sufficient to cause horses to reduce speed and stride length. The most common cause is high grain-low roughage diets.
Lameness can also occur with cases having been reported of cancer and melanoma infiltration into the sacral nerves, spinal cord and muscle fibres. Other less easily diagnosed causes of lameness include muscle and bone disorders associated with nutrition, infections, immune-mediated disorders, toxins, inherited myopathies (disease of muscle tissue), endocrine problems (including pars pituitary intermedia dysfunction - PPID), liver disease, pasture-associated, malignant hyperthermia (severe reaction to medication during anaesthesia), tying-up and nutritional secondary hyperparathyroidism (high concentration of parathyroid hormone in the blood due to calcium deficiency).
Disorders affecting the peripheral nerves (those outside the brain and spinal cord) result in denervation and muscle wastage. Any abnormalities in the tendons, bones, bursa or ligaments in the navicular area can cause mild-to-severe chronic lameness. There is not a single gold standard for mild lameness detection and clinical signs cannot accurately predict navicular bone disease or other injuries in the navicular syndrome. MRI is often the best tool.
GAIT ABNORMALITIES
There are several unusual gait abnormalities that include ‘shivers’, stringhalt, sweeney, tetanus and dropped elbow.
Australian stringhalt is associated with ingestion of dandelion flatweed and cheeseweed. The second form of stringhalt may be associated with injury to the stifle, hock, back cannon bone, upward fixation of the patella and painful foot conditions. Other disorders of the muscle-tendon unit that cause gait changes include exertional rhabdomyolysis (tying-up), PSSM, fibrotic myopathy, peroneus tertius rupture, upward fixation of the patella and lacerations of the superficial and deep digital flexor tendons and suspensory ligament.
Fortunately, about 70% of lamenesses resolve. Successful resolution without proper diagnosis and treatment is the predicament, so understand the veterinary lameness exam and the full-range of diagnostic aids. Always work with the veterinarian to diagnose problems early so appropriate and effective treatments can be used. Most importantly, recognise the value of a veterinary diagnosis. A methodical clinical veterinary exam will always be the cornerstone of lameness diagnosis. Treatment without diagnosis can, in some cases, be a waste of money, time and resources – and it can compromise your horse’s well-being and future soundness.
ABOUT THE AUTHOR
Dr Jennifer Stewart BVSc BSc PhD MRCVS Dip BEP AAIM
Equine Veterinarian and Consultant Nutritionist
An equine veterinarian with over thirty five years’ experience, Jennifer is also a consultant nutritionist and has formulated feeds, custom mixes and supplements for leading international horse feed manufacturers in Australia, India, Ireland, Japan, New Zealand, Philippines, South Africa, Thailand, Turkey and the UAE. Dr Stewart is passionate about equine nutrition and its role in the management, treatment and prevention of many equine disease and she is committed to bringing ‘science to the feed bin’.
For more information visit web: www.jenquine.com |
|
 |
 |